Sleep Apnea
Obstructive Sleep Apnea Syndrome (OSA) is an under-diagnosed condition. It affects about 300 million people in Organisation for Economic Co-operation and Development (OECD) countries. The consequences of this pathology can be serious, particularly on cardiovascular health, road accidents, diabetes, etc. OSA results from the obstruction of the pharynx by the tongue.
Description
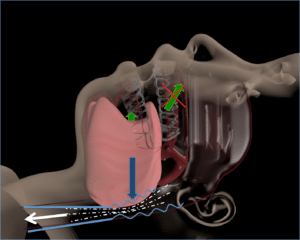
Like snoring, Obstructive Sleep Apnea is caused by a receding position of the tongue and its lack of tone during sleep. This position is related to the dysfunctions of the tongue that has not acquired the right landmarks in the mouth. In addition, its dysfunctions during the day lead to muscular fatigue which induces too weak a tone during sleep. These combined factors lead to insufficient tension of the lingual and pharyngeal membranes.
The tongue retreat during sleep will cause a narrowing of the diameter of the pharynx. The extra inspiratory effort required to attract air into the lungs leads to increased depression in the pharynx, which will increase the attraction of the tongue backwards. Under these conditions, the toned tongue cannot resist and partially or totally blocks the passage of air. This results in episodes of respiratory arrest during sleep. In most cases, the patient wakes up for a fraction of a second (microwave), re-opens his pharynx by moving his tongue forward and opening his mouth to breathe in quickly to fill his lungs, swallows, falls asleep.
Obstructive Sleep Apnea is promoted by oral breathing, overweight, back position or aging.
Symptoms
It is possible to detect Obstructive Sleep Apnea. A person who snores regularly is likely to have apnea. Breathing stops during sleep are apneas. Fatigue upon waking, falling asleep during the day, irritability, difficulty concentrating, high blood pressure is other symptoms of Obstructive Sleep Apnea. If so, talk to your doctor.
In children, attention should also be paid to the quality of sleep, including breathing through the mouth, snoring, stopping breathing, frequent awakening, agitation, nightmares, sweating, abnormal movements, somnambulism or “bedwetting”. In this case, do not hesitate to consult a specialist to diagnose the pathology and set up an appropriate treatment.
A nocturnal sleep recording will be made to determine the type and severity of the disorder.
Consequences of Obstructive Sleep Apnea
Severity designations are different for adults and children, as the consequences are always more serious when problems occur early. They are also dependent on countries. In France, apnea in children is considered moderate beyond one apnea per hour and severe beyond five per hour. In adults, OSA is considered a “moderate” pathology from 15 apneas per hour. Beyond 30 apneas per hour, it is considered severe.
Insufficient oxygenation (hypoxia) of the body caused by Obstructive Sleep Apnea can lead to potentially serious pathological consequences. They can result in increased risks of cardiovascular complications (hypertension, heart attack, stroke…), metabolic complications (diabetes, obesity…), neurological complications (depression, libido disorders…). According to studies, the risk of cardiovascular accident in patients with Obstructive Sleep Apnea is 30 to 70%.
The respiratory microwaves prevent the patient from reaching the phases of deep, REM sleep and their regenerative functions. You then feel very tired during the day. It is harmful to attention, intellectual productivity and very dangerous when driving a vehicle, train or machinery!
In children, the consequences are particularly important for their physical and intellectual development. In addition to sleeping poorly and waking up very tired, he has difficulties with attention and concentration, which he compensates for by an unbearable hyperactivity for those around him. Insufficient oxygenation (hypoxia) of the brain can have irreversible repercussions on its future intellectual development.
Prevalence
Recent studies show that more than 20% of children have Obstructive Sleep Apnea syndrome. A research team has shown that in adults, 25% of women and 50% of men aged 30 to 60 have more than 15 apneas per hour of sleep. Contrary to popular belief, weight is not a decisive factor for nearly half of these patients. This pathology could therefore affect more than 300 million people in the 35 OECD countries. Most people with it are unaware of this. Most often it is the people around you who detect the first signs: loud snoring punctuated by respiratory stops and brutal repetitions.
Studies have shown that 50% of men and 25% of women have Obstructive Sleep Apnea.
Treatment
Adequate treatment should allow the upper airways to be cleared and air to pass unobstructed. It should also act on the cause of Obstructive Sleep Apnea, not only on its consequences: the tone and position of the tongue. This is the only way to maintain the opening of the pharynx over time, not only when a device is worn. In addition, it should not exert forces on the teeth, as this would force them to change their position in the medium term and could lead to undesirable effects. Finally, the more comfortable, non-invasive, discreet… the device is, the more likely it is to be well tolerated by the patient. This high compliance is of course crucial to achieving results during treatment.
Lingual reeducation is the only treatment with long-term healing potential for Obstructive Sleep Apnea. Several studies conducted in Europe, North and South America have shown interesting results by acting on lingual dysfunctions: the main cause of Obstructive Sleep Apnea.
Doctors have achieved a 30% decrease in apnea indices after only 60 minutes of daily exercise for one week. This type of treatment could be offered alone or in addition to a PPC. This reeducation requires the commitment of the patient and the therapist. Its development would be facilitated in the case of standardized treatment.
To learn more about the reeducation management of OSA, discover the articles written by Mr. Vanpoulle, Physiotherapist-Osteopath specializing in maxillofacial therapy, and member of the Tongue Lab scientific committee: article on Kiné Actu
Lire les autres chapitres :